
TEMP: Enabling Surgeons With Patient-Specific Guides: A Computational Design Journey
Interview with Or Benifla – CustoMED.ai
Or Benifla, co-founder of CustoMED.ai, is helping reshape surgical workflows by placing computational design tools directly into the hands of surgeons.
In this interview ahead of his presentation at CDFAM Amsterdam, he explains how his team built a modular, AI-accelerated platform that automates the design of patient-specific surgical guides—without requiring CAD expertise.
Drawing on clinical data from Sheba Medical Center and a deep understanding of surgical planning, CustoMED’s tools allow clinicians to interact with intuitive web-based interfaces built on Grasshopper and ShapeDiver, enabling rapid iteration, validation, and production.
Benifla shares lessons learned from scaling in regulated environments, the importance of balancing surgeon control with compliance requirements, and case studies showing how CT-to-print pipelines can now operate within hours, not weeks.
The result is a faster, more accessible approach to personalized medicine that remains grounded in clinical realities.
Your company focuses on making personalized surgical tools more accessible. What specific challenges in the current surgical design process motivated the development of your platform?
The surgical design process today is highly fragmented and relies heavily on manual operations. Engineers often jump between disconnected software tools, with significant back-and-forth communication required between clinical teams and technical designers. Much of the work is repetitive and error-prone. This not only introduces delays but also limits scalability and increases the barrier to entry for wider clinical adoption.
I saw an opportunity to streamline this entire pipeline by building an end-to-end platform that automates the critical steps while keeping the surgeon at the center of the process.
The goal is to reduce the need for designer/ engineer intervention, ensure consistency in design quality, and ultimately make personalized surgical tools more accessible and clinically practical.
How did you acquire the training data needed to develop your system, and what was required to ensure the approach was robust and intuitive enough for non-CAD experts, like surgeons, to trust and adopt in clinical practice?
We spun off from Sheba Medical center, naturally gaining access to twenty years of clinical data and unlimited operating-room access.
That rich dataset formed the backbone of our training pipeline, while ongoing collaborations with additional hospital labs worldwide allowed us to validate and refine our models against diverse anatomies and surgical workflows.
Working as a multidisciplinary team; designers, software engineers, clinical specialists, and human-factors experts in the operating theater, we continually anchored our development process in real-world practice rather than abstract CAD exercises.
Ensuring robustness and intuitiveness meant more than just high-accuracy algorithms; it demanded that surgeons feel in control at every step.
Drawing on years of hands-on jig development, we distilled our collective know-how into a suite of modular “surgical apps” that share a common AI foundation.
For example, our automatic segmentation and landmarking engine for the lower limb becomes the starting point for: ankle-replacement, knee-realignment, or deformity-correction guides, each app encapsulates all the surgical planning logic, recommended structures, and preferred design configurations tailored to the specific pathology.
By packaging complex geometry workflows into familiar, game-like interfaces and providing clear visual feedback at every stage, we give non-CAD experts the confidence to prepare and customize their own guides, knowing that the system reflects decades of surgical best practice.

What advice would you give to others trying to build computational design tools for highly specialized, regulated domains like surgery? Where do you think it’s most important to start—and where are the potential pitfalls?
As cliche as it may sound – you have to embrace the attitude of constant iteration and very high friction with the target users. Those kinds of processes aren’t obstacles; they’re your roadmap to the creative workarounds that make your MVP both lean and laser-focused.
By leveraging products and platforms – like ShapeDiver for parametric models – you can expose early concepts to real users in days rather than months.
Seeing your tool in the hands of surgeons, watching how they manipulate parameters in real time, helps you distill an intuitive UI, funnel complexity out of the workflow, and fine-tune your algorithms against genuine clinical scenarios.
I think the biggest pitfall in computational design initiatives is misaligning incentives between the end-user and the purchasing stakeholder.
Surgeons crave control, hospitals prioritize validation and return on investment, and regulators demand traceability.
Navigating this “product tango” means building a bridge in a framework that delivers confidence and compliance, while preserving the surgeon’s sense of authorship. Overlooking any one party’s needs can leave you with a beautiful prototype that never secures clinical adoption or a purchasing decision.
The key is to balance agility with structure iterate relentlessly, but always underpinned by rigorous documentation and real-world feedback loops that satisfy both regulatory requirements and the surgeon’s expectation for precision.



Reverse shoulder arthroplasty for a chronic anterior dislocation at Angeles Querétaro Hospital using a fully digital workflow—powered by CustoMED posted by Alberto Guevara Alvarez on Linkedin, May 20, 2025
What does your development stack look like—from CAD and reverse engineering to integration with surgical planning tools? How do you structure data input and output across this pipeline?
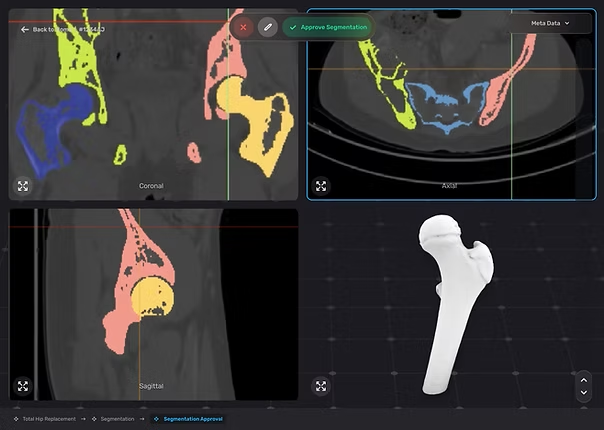
Our development stack is built for modularity, speed, and clinical reliability. We start with segmented anatomical data, derived from CT scans, then after building a design prototype we usually find ourselves in the O.R understanding the usage of the tool and realizing the broader picture of the surgical technique.
From there, we build a fully parametric system using Rhino and Grasshopper as the backbone for all geometry creation, and ShapeDiver for the interaction with the end user – the most important thing.
Each module in the workflow, Segmentation, landmarking, implant positioning, is developed as a standalone computational design routine. Data tagging -> machine learning pipeline, the PSI design segment is a classic algorithm. This allows us to fine-tune and validate each piece individually, which is key for accuracy but also regulatory robustness.
On the input side, we take Ct scans (DICOMS) and surgical preferences. The output is always a 3D printable file, but we also generate surgical planning reports, PDFs for the OR, and internal logs for traceability and quality control.
Everything is built with API compatibility in mind, so we can integrate with hospitals’ PACS systems from the input side, cloud platforms for planning and analysis in the future and even directly with 3D printers.
In our previous conversations, you mentioned using Grasshopper and a modular, iterative development approach. How has this influenced your ability to scale or respond to clinical feedback?
We use Grasshopper mainly in the surgical planning and PSI design phases. It’s our playground for fast iteration.
Sometimes, we’ll prototype an automated surgical app or planning tool in Grasshopper, and even though it’s not fully baked, it lives on in that intermediate state because it solves real problems and the shapediver integration gives clinicians a tangible, usable interface.
One of the biggest advantages is how quickly we can test ideas. What might take weeks to code properly dealing with bugs, exceptions, UI logic we can simulate in a day in Grasshopper. That means we can validate concepts, show results to users, and only then decide if it’s worth investing in full development.
It’s also saved us countless hours by helping us avoid dead ends. Once you put a coded feature in front of a user, they’ll immediately ask for changes and if you’ve already overcommitted technically, that’s a problem. Grasshopper gives us that buffer to explore, adjust, and evolve with real clinical feedback
What case studies or clinical collaborations best demonstrate how your tools are being used in real-world surgical workflows today?
We have three very different case studies that show how our tools are being used in real-world surgical workflows – and they each demonstrate a different strength of the platform
First is Sheba Medical Center in Israel.
Because they have a 3D printer in-house, we’ve been able to completely transform how they handle trauma surgeries. We’re talking about going from CT to a surgical guide in hand within two hours. That kind of turnaround used to be unthinkable. It’s not just about speed – it’s about removing friction to the point that surgeons don’t even hesitate before using the system. It becomes second nature.
The second example is from India, where we collaborated with a local service bureau on a cranial implant cases.
What’s remarkable here is that the entire pipeline – from CT to implant design – ran fully automated. No human touched the design. The surgeon just went through the interface ‘Next, Next, Next’ – and got a ready-to-print implant. It shows what’s possible when you remove complexity and build real trust in automation.
And finally, we’re working with a German implant manufacturer probably the most conservative and compliance-driven client you can imagine. They’re now going all-in, implementing four dedicated surgical apps using our platform.
Together, these collaborations prove that whether you’re operating inside a hospital, partnering with a service bureau, or integrating into a global manufacturer’s workflow – when solving the right problems – it’s easy to adapt – you scale.
What key points will you be sharing at CDFAM Amsterdam, and what kind of feedback or conversations are you hoping to have with the CDFAM community?
At CDFAM Amsterdam, I’ll be sharing the truth – I’m here to learn.
I love the idea traffic. That back-and-forth is where the real value happens, and CDFAM is one of the rare places where people from all corners of the industry are in the same room. And then we’re all eating pretzels together in the other room. That’s the perfect setup to challenge our assumptions and stress-test our system.
So I’m looking forward to connecting with as many people as possible, and to the kind of multidisciplinary conversations that push things forward faster than any echo chamber ever could.
Register to attend CDFAM Amsterdam 2025 and connect with Or Benifla and others leading the development of computational design tools across industries. Join the conversations shaping the future of design, engineering, and advanced manufacturing.






